What’s Your Standard Operating Procedure (S.O.P.)?
At Movement As Medicine, we pride ourselves on “treating the person” not “treating the pain.” We’ve worked to develop a treatment system not only to identify the best approach in the clinic but also how to best educate and empower our clients to manage their health outside of our doors.
We stress the importance of a “client driven” treatment process. As clinicians we work as “treatment leaders” shifting responsibility to the client to ultimately manage his or her own health through physical activity.
As strength and conditioning coaches, we are always treating clients with the end goal of exercise and physical activity in mind. In our mind no “rehabilitation program” is complete if it does not address fitness.
We utilize manual therapy and motor control training as a means to improve movement quality and open more windows of opportunity for exercise. It is our mission to help people move and feel better so they can be physically active and get back to doing whatever it is they love to do!

A few notes to address before we get into what we do at MAM:
1. If you’re taking the time to sit down a read this we assume you are someone with a very open mind, who enjoys learning from others. What we’re about to show you is why & how we do what we do. If you do it differently, that’s cool with us! As long as you get results & you’re doing everything you can to help the individual in front of you, keep going. All we ask is you take what we do and apply it to your own model where you see fit. Do NOT try to copy us. That is a recipe for disaster. This is our interpretation of everything we’ve been exposed too. We share this information to encourage you to evaluate your own treatment/training model. Ask yourself the question: “what could we/I do better”. We are always adding to our “toolbox”. I’m sure there’s plenty we could learn from you.
2. If you don’t know REFER OUT! We are strength coaches and personal trainers NOT doctors or physical therapists. We do not make medical diagnoses. Some things are a medical problem and some things do need surgery! Not everything is a “movement” dysfunction or a fitness fix. Anything that is painful please refer to a doctor or specialist in your area. Do your best to make that person part of your network as it’s about helping the individual, not about egos. In the end everybody should win; you, the doctor, the therapist, and most importantly the client. Sometime we even front the cost for our client to go and see someone else. Don’t worry, if you show enough love to pay for them to see someone of a different skill set than you they will come back. They’re a client for life.

3. You can always be training something! If the only thing you can do is a half kneeling press on one arm and ride the bike, then do those two things… A LOT! The positive systemic benefits of exercise on the human body aids in the rehabilitation or improvement of (X) body part or segment even if you are not training it directly. Movement is Medicine.
Look at this list of positives from exercise & movement:
http://www.sleeplikethedead.com/exer-100benefits.html
We hope this gets our point across. You’ll only speed up the healing process by training what you can.
With that said, here’s how we do it at MAM:
Health History/ Subjective/ Questionnaire
We start all of our initial sessions with a health history & questionnaire. We ask questions about everything; current symptoms, nervous system, medications, lifestyle, breathing, jaw, teeth, pelvic floor, childhood sports and previous injuries. We use all this information to create a holistic plan based off of the individual.
Then we take subjective feedback AKA listening, engaging, and empathizing with the client. This is part of the reason, we believe, our clients; love coming back, listen to what we have to say, and refer us to all their friends. Does that mean we act on all of their problems? No. We still use our systems, but we do listen to their story. We don’t make assumptions about their pain and how they perceive it. We want them to feel comfortable. In my observation many clinicians, trainers, and therapist miss this important step or dub the information as arbitrary. Emotions and psychology play into someone’s physical healing as much, maybe even more for some, as biology. Think placebo effect.
Assessment
“If you’re not assessing you’re just guessing.”
You have to have an assessment. We don’t care what it is, just have one. No need to argue over what’s better or what’s worse. It doesn’t matter. As long as you have one, you use it consistently, and your clients get better.
Our assessment?
Pain = Selective Functional Movement Assessment (SFMA)
No Pain/Return to Play = Functional Movement Screen (FMS)
We use the FMS and SFMA because of their systematic approach. It’s simple, we’re comfortable with it, and we get results.
Don’t like the FMS or SFMA? Or you think it doesn’t work? That’s ok, these are the tools that work best for us, in our setting. We can’t believe people waste time arguing on the internet about this stuff. What we should all be worried about is the person in front of us and if we can help them or not. Do you have an assessment? Do you use it? Have you mastered it? Do you re-test to see if you’re getting results? Do you get people better? Do you refer out when necessary? If you have your own system or you use the orthopedic model that’s great! Become a master of the model you prefer (principals) and add in what entices you (methods) from other systems as you see fit.

“The lens we see treatment & movement through”
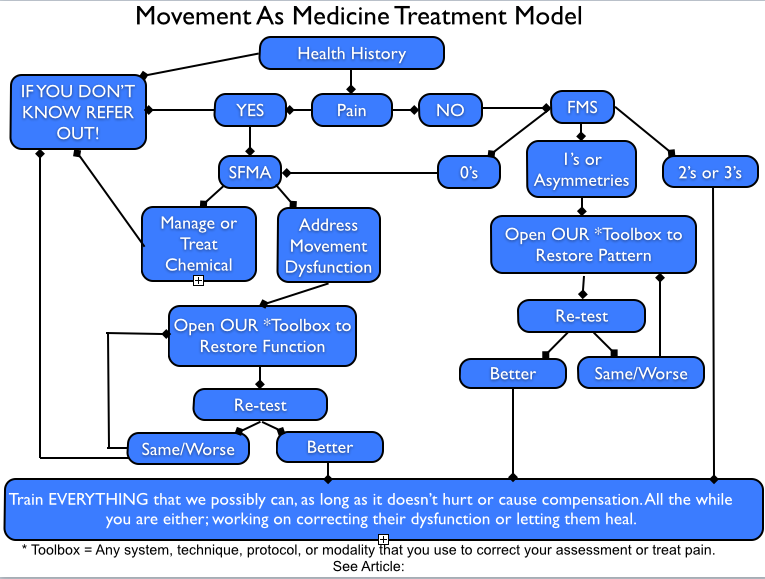
Below are the options the systematic approach of the SFMA & FMS can lead us too:
SFMA
- Manage and treat pain (we refer this out) OR
- Address movement dysfunction OR
- Do Both
FMS
- 0’s = SFMA (see above)
- 1’s and Asymmetries (a 1-3, 2-3, or a 1-2) = address with your toolbox (see below). **Remember the body is asymmetrical. We’re looking for significant asymmetries, not minute differences.
- 2’s or 3’s = Train these patterns and train ‘em HARD
Toolbox
This is anything you use to correct your assessment & improve movement. We are not here to say one system or treatment is better than another. Who cares?
“If you spread peanut butter on their back and they improve then you chose the right treatment for that person at that time.” – @CWagon75
Our toolbox includes; Massage Therapy, IASTM, FMS correctives, the 4X4 SFMA matrix, Neuro Kinetic Therapy, Functional Anatomy Palpation, Functional Range Conditioning, MovNat, The MBSC & CFSC System, Postural Restoration Institute, Rocktape, Original Strength… we are also huge followers of Kelly Starrett’s Mobility WOD, Charlie Weingroff’s Training=Rehab DVD’s, everything Dan John, Eric Cressey, & Pavel have put out.….. As you can see we are not tied to any one system or thought pattern. Whatever is best for that specific situation, we use it! We don’t care who “invented” it. Who pushes it. Who teaches it. Who gets the credit. If it works and gets the job done then that’s the treatment or assessment we use for the individual. If it doesn’t work, we go back into the toolbox try something else. It doesn’t need to be rocket science. Pull from your collective experience and treat. Fail and try again until you succeed or make the call to the bullpen.
![]()
“The lens we see training through”
***Courses and systems we are not as familiar with, but have been exposed too, and are certainly a viable treatment option for your toolbox; Dynamic Muscular Stabilization, RKC, StrongFirst, Tri-phasic training, Westside Barbell, Crossfit, EXOS (Athletes Performance), NASM, NSCA, NPTI, Omega Wave, Chiropractic, World Athletic Center, Titleist Performance Institute, 5/3/1, Juggernaut Training Systems, DeFranco’s, NeuroMuscular Massage Therapy, Muscle Energy Technique, Cupping, Fascial Manipulation, Mulligan Technique, Dry Needling, Graston, USA-Weightlifting, Animal Flow, Yoga, Proprioceptive Neuromuscular Facilitation, The Hendrickson Method, Active Isolated Stretching, Primal Move, Proprioceptive Deep Tendon Reflex, Anatomy in Motion, Rolfing, Active Release Technique, Egoscue, Z-health, Feldenchrist, the list goes on and on!! There are a thousand ways to skin a cat, find the best ways that work for you.
If you’re toolbox isn’t big enough, don’t be afraid to refer out, or take a course. More keys on the key ring wins. *Hint: The smart people in your network also count as “keys” on your key ring. Please don’t waste your time & client’s money by guessing. It’s ok to not know. Work on your network of like minded professionals, and find people you can trust in your area. We know doctors, physicians, surgeons, orthopedists, naturopaths, podiatrists, physical therapists, chiropractors, acupuncturists, dentists (Why dentists? That’s another blog post for another time. Check out PRI’s Cervical Revolution course. You’re teeth are sensory organs) We can call or email these people at any time to get our client in the correct hands.
Side note: Medical Treatment Protocols include – ice, heat, electric stim, medications, topical creams, muscle relaxants, NSAIDs, cortisone, ect…. Basically anything that will affect chemical pain, decrease swelling & inflammation of the injury. At MAM we do not do or recommend medical treatments. We know what we don’t know. We are strength coaches who use manual therapy to change movement. Not doctors. If they’re coming off a surgery usually they’ll be working with a physical therapist first, and a fitness professional second (and we can only hope at the same time!).
We also include nutrition in this category…. be sure to find a nutritionist who understands athletics, exercise progression, injury, monitoring, other recovery measures, & the importance of continuing education. They go hand in hand and a good one will understand all six. If it’s a medical issue we recommended a registered dietician or a naturopath. For basic nutritional & recovery needs with a clear medical history we recommend Precision Nutrition or Chek Practitioners. Remember to refer out if need be!

“More keys on the key ring wins.”
Test/ Re-test
Re-evaluate your audit – did it work? Yes or no? SOOOO many trainers and therapists do spot on assessments, perform wonderful treatments, write up a great program, and then skip this important step. Always re-evaluate. If you’ve picked the correct intervention there should immediate change. If you’ve run out of time for that days treatment session send them home with breathing (I haven’t had many people get on the table who couldn’t benefit from some breathing practice and relaxation. Check out all the benefits of learning to breathe here. You’re not going to exacerbate the problem by laying on your back and breathing.) and re-evaluate again the next time they’re in, digging back into your toolbox for the next thing.
Integration
There are two parts to this:
1. Back up your work. If you give someone new found mobility or stability get them to use it! (We almost always try to do this with exercises that are self-limiting) Re-train the brain and body to accept the changes you have made, and remember, this does not happen in one session.
Ex. Assessment Shows Limited Ankle Dorsiflexion on One Side – Manual Input on Ankle to Reset Range of Motion – Ankle Progressive & Regressive Angular Isometrics To Reinforce – Deadlift & Farmer Carry to Reload
It take multiple inputs over a long period of time to induce change. Any who says “I can fix you in one session” is a liar and a witch doctor. Get your money back. The one shot kill is “cool” to watch but if it doesn’t stick as soon as they stand up you’ve done nothing. Yes you may feel better after, but if you don’t do the work consistently with intent then it will keep coming back.

2. Train everything you can, that doesn’t hurt or cause compensation, and train progressively with resistance while you either work on correcting their dysfunction or let them heal. We love this Charlie Weingroff quote from Training = Rehab which was the motivation for his new DVD Lateralizations and Regressions.
“There is no rehab. There are only lateralization and regressions from you’re your best program.”
Write out the exact program you think this person should be doing for whatever they’re goal. If they were 100% healthy what would their program look like? Print it out. Then go through it and either regress (take a step back to something easier, you go down a level) or lateralize (to take a side-step to something similar and you stay on the same difficulty level) everything that will affect their pain or dysfunctions. If it hurts don’t do it. Then start slowly working them towards the finish line. “Simplicity is the ultimate sophistication”. This is exactly how we train our athletes at MBSC, work with all our clients at Movement as Medicine, and is the basis of our Certified Functional Strength Coach course.
Conclusion
In the end the #1 thing we do is educate. We teach our clients to treat themselves. It takes multiple inputs over a long period to time to get someone to move better and make change. How does someone do this? On their own time! We cannot walk around with you massaging and stretching your quads all day long. That would be exhausting and cost you quite a bit of $. But you can certainly do it yourself. We only have people come in to see us so we can expedite the process and progress their exercises, but it’s on them to do the work! You are going to make YOURSELF better. The patient needs to do their own healing. We are here to guide them through it and make sure everything that needs to be in place, is.
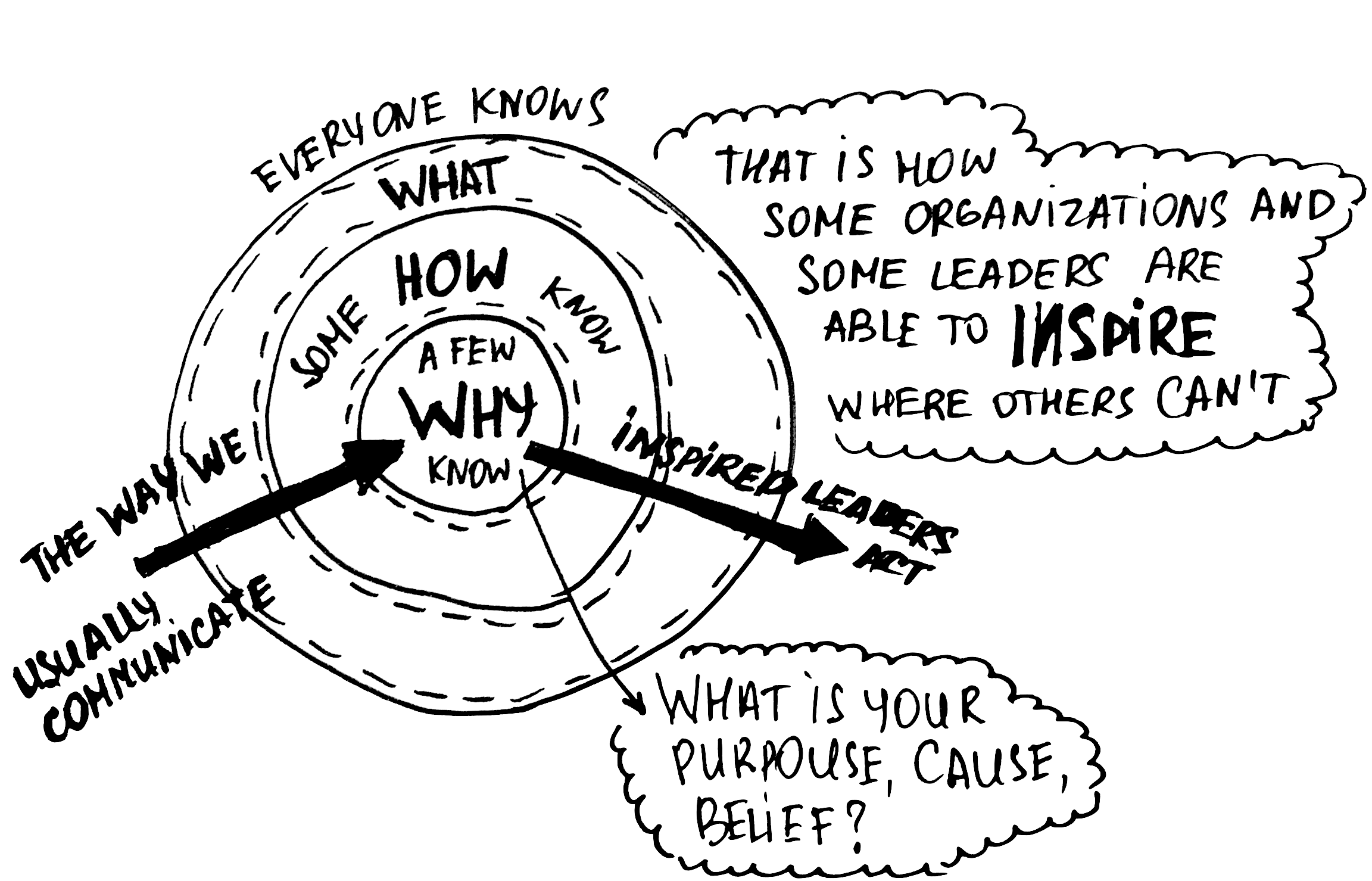
What it comes down too is we are more than strength coaches, therapists, trainers…. We are teachers. We teach because our goal is to see you better in the least amount of visits possible and instead out doing what it is you love to do! Some would say “What a horrible business model!” We would argue… “When people buy what you do and WHY you do it they;
- don’t stop talking about you to all their friends.
- aren’t hesitant to give you their money.
- and even when they are better they come back for maintenance! It’s like a cleaning at the dentist. Come back every 3 to 6 months to make sure they are on track.
We aren’t in it for the money. We’re in it to help people move better so they can do what it is they love and enjoy life.
What is your WHY?
If you would like to learn more about what we do please follow us on Facebook, Twitter, Instagram, or attend a CFSC or one of our mentorships.
This article was written by Movement As Medicine co-owner and CFSC Coach Brendon Rearick. He can be contacted at brendonrearick@gmail.com